Dr. Michael Zellner began his medical career in 1988 as a urologist at the urological clinic and polyclinic of the Ludwig Maximilians University hospital (Klinikum Grosshadern) in Munich. His research focus there was bladder dysfunctions and erectile dysfunctions with a wide range of causes.
Until the end of 1995, he headed the scientific working group “Urodynamics and Neurourology” and established one of the first specialized clinics for bladder dysfunctions at Klinikum Grosshadern. The importance and necessity of professional, specialized urological rehabilitation became increasingly clear to him, with the medical community’s general lack of interest in the necessary differential diagnosis and treatment of bladder dysfunctions, and the frequent use of intense surgical interventions, especially radical prostatectomies and cystectomies.
In 1996, under his professional leadership, the first clinic for specialized urological rehabilitation was opened in the Lower Bavarian town of Bad Griesbach im Rottal. This clinic developed rapidly and successfully, later going on to become the Department of Urology and Neurourology at the Johannesbad Fachklinik Bad Füssing on July 1, 2010. There, a multidisciplinary team of experienced specialists in urology along with specially trained therapists and nursing staff continues to provide treatment for patients with disorders of sexual function and the bladder, among other things, on an inpatient and outpatient basis according to a multimodal treatment concept.
For around eight years now, muscle stimulation of the pelvic floor region with the QRS PelviCenter has been an integral component of this successful treatment concept. A crucial factor in the productive treatment of bladder dysfunction is isolated flexing of the pelvic floor musculature, both under stress conditions and the occurrence of symptoms of a hyperactive bladder (frequent urination, nocturia = urination at night, an imperative (unsuppressible) urge to urinate, with or without urinary incontinence = unwanted discharge of urine (OAB syndrome = “over-active bladder,” formerly called “urge incontinence” or “irritable bladder”).
To avoid “faulty feedback” in the central nervous system in such cases, simultaneous flexing of the frequently incorrectly utilized buttock, thigh, and abdominal muscles (“auxiliary musculature”) must be avoided. However, it is particularly these muscles that are very frequently activated by affected patients, as they are unaware of the existence and controlled flexing of the relevant pelvic floor musculature. Learning and training of targeted, coordinated flexing of the pelvic floor first requires adequate awareness training. Ideally, success is achieved through regular vaginal or rectal palpation by a therapist who is well-trained and experienced in this technique. This is to be done during the entire active pelvic floor contraction training sessions, which are conducted regularly.
Comparably good results for awareness of these important muscle groups can also be achieved using the PelviCenter, however. Without having to undress and be touched in intimate areas, the patient receiving treatment will feel the rhythmic contractions in the pelvic floor (= continuous awareness training). Regular application results in the necessary increase in strength and stamina (“bodybuilding” for the pelvic floor), but without the patient having to exert an extraordinary amount of force. Hence, when used in an isolated fashion or in combination, the PelviCenter can lead to the (significant) alleviation or elimination of corresponding dysfunctions.
Among other things, the high level of acceptance, effectiveness, and subjective positive reviews during treatment with the PelviCenter are under continual objective evaluation as part of the quality assurance measures of the Department of Urology/Neurourology at the Johannesbad Fachklinik. The findings have already been presented at professional conferences.
According to Dr. Zellner, one other increasingly important advantage of treatment with the PelviCenter is the increasing scarcity of cost-intensive “human resources.” Already today, there are an insufficient number of interested doctors and qualified therapists available for the long-term treatment of bladder and sexual dysfunctions. In Dr. Zellner’s opinion, consistent and sufficiently long treatment (approx. two sessions weekly with a total of at least 10 to 15 applications) with the PelviCenter is in many cases a good option for alleviating or even healing symptoms conveniently and discreetly, even in cases where no treatment was desired or possible to date. However, if even after this period of treatment using the PelviCenter, no satisfactory improvement in symptoms is observed, he recommends that patients be referred to a urological specialist in order to investigate possible causes and not overlook possible risk factors.
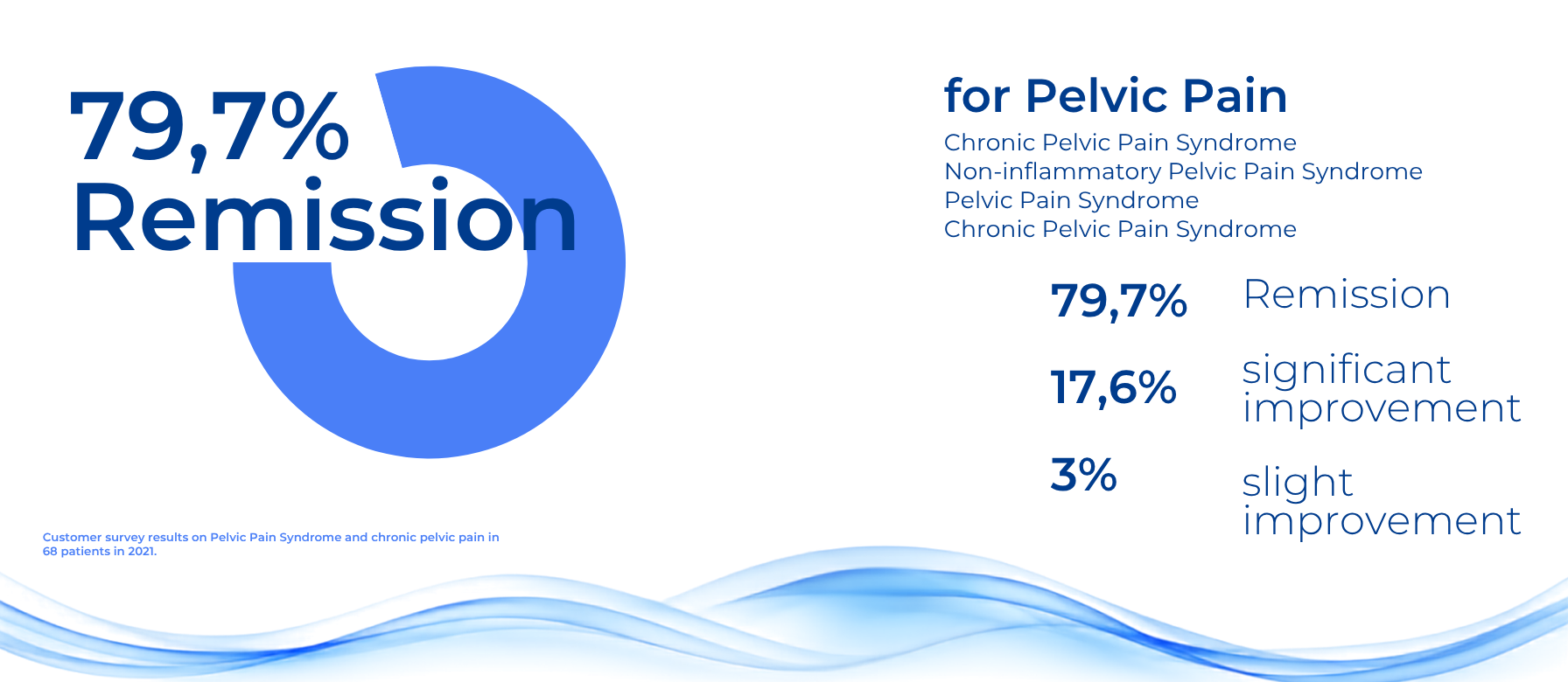
Furthermore, QRS muscle stimulation can also achieve positive results in the case of chronic pain in the pelvis minor region (“pelvic pain syndrome”) and erectile dysfunction. Clinical studies currently in progress on these conditions are expected to provide further scientific support for the effectiveness of the clinically observed successes of the treatment.
Dec 6, 2017, © QRS-International AG